
A New Weapon in the War on Cancer June 2023 Issuer Free Writing Prospectus Filed pursuant to Rule 433 Registration Number 333 - 260565
Safe Harbor and Forward - Looking Statements 2 Intensity Therapeutics, Inc . (the “Company” or “we”) has filed a registration statement, including a preliminary prospectus, with the U . S . Securities and Exchange Commission (the “SEC”) (File No . 333 - 260565 ) in connection with the offering to which this presentation relates . Sales of the securities of the Company offered pursuant to the registration statement may not be made or offers for such securities accepted prior to the registration statement becoming effective . Before you invest, you should read the registration statement, the preliminary prospectus included within the registration statement and other documents the Company has filed with the SEC for more complete information about the Company and this offering . You can obtain a copy of the preliminary prospectus for free by visiting EDGAR on the SEC website at www . sec . gov . Alternatively, the Company will arrange to send you the preliminary prospectus, which you may request by emailing jwesolowski@intensitytherapeutics . com . This presentation may not be reproduced, forwarded to any person or published, in whole or in part . The Company is not soliciting offers to buy securities of the Company in any jurisdiction where the offer or sale is not permitted . This presentation contains forward - looking statements within the meaning of The Private Securities Litigation Reform Act of 1995 that involve substantial risks and uncertainties, including statements regarding the development and regulatory status of our product candidates, such as statements with respect to our lead product candidate INT 230 - 6 , and the timing of clinical trials and data from those trials for our product candidates, and our discovery programs that may lead to our development of additional product candidates, the potential utility of our technology and therapeutic potential of our product candidates, the potential commercialization of any of our product candidates, and the sufficiency of our cash resources . All statements, other than statements of historical facts, contained in this presentation, including statements regarding our strategy, future operations, future financial position, future revenues, projected costs, prospects, plans and objectives of management, are forward - looking statements . The words “anticipate,” “believe,” “estimate,” “expect,” “intend,” “may,” “might,” “plan,” “predict,” “project,” “target,” “potential,” “will,” “would,” “could,” “should,” “continue,” and similar expressions are intended to identify forward - looking statements, although not all forward - looking statements contain these identifying words . We may not actually achieve the plans, intentions or expectations disclosed in our forward - looking statements, and you should not place undue reliance on our forward - looking statements . Actual results or events could differ materially from the plans, intentions and expectations disclosed in the forward - looking statements we make as a result of various risks and uncertainties, including but not limited to : whether we will be able to successfully conduct Phase 1 , 2 or 3 clinical trials for INT 230 - 6 , whether we complete other clinical trials for our product candidates, whether we receive results from our clinical trials on our expected timelines, or at all, whether our cash resources will be sufficient to fund our foreseeable and unforeseeable operating expenses and capital expenditure requirements on our expected timeline, whether the COVID - 19 pandemic impacts our operations, and other factors included in the “Risk Factors” section of the Company’s filings with the SEC in the future . Any of these outcomes could cause our actual results to differ from those contained in the forward - looking statements of the Company’s filings with the SEC . The forward - looking statements contained in this presentation reflect our current views as of the date of this presentation with respect to future events, and we assume no obligation to update any forward - looking statements except as required by applicable law . The Intensity Therapeutics, Inc . name and logo are our trademarks . We also own the service mark and the registered U . S . trademark for DfuseRx . The trademarks, trade names and service marks appearing in this presentation are the property of the Company . We have omitted the ® and Ρ designations, as applicable, for the trademarks named in this presentation .
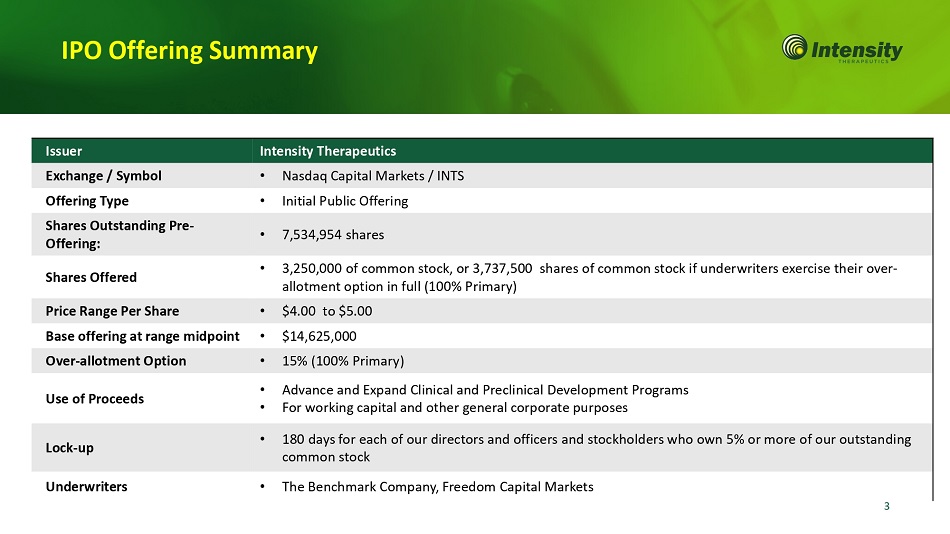
Intensity Therapeutics Issuer • Nasdaq Capital Markets / INTS Exchange / Symbol • Initial Public Offering Offering Type • 7,534,954 shares Shares Outstanding Pre - Offering: • 3,250,000 of common stock, or 3,737,500 shares of common stock if underwriters exercise their over - allotment option in full (100% Primary) Shares Offered • $4.00 to $5.00 Price Range Per Share • $14,625,000 Base offering at range midpoint • 15% (100% Primary) Over - allotment Option • Advance and Expand Clinical and Preclinical Development Programs • For working capital and other general corporate purposes Use of Proceeds • 180 days for each of our directors and officers and stockholders who own 5% or more of our outstanding common stock Lock - up • The Benchmark Company, Freedom Capital Markets Underwriters 3 IPO Offering Summary
Investment Highlights • Novel Approach to Immuno - Oncology with First - in - Class Compound that causes cancer cell death leading to an immune response for indications with high unmet medical need • Multiple Late - Stage Pipeline Programs in the Clinic across metastatic and presurgical settings with multiple near - term inflexion points • Experienced Leadership Team from Emisphere, Roche and Bristol Myers; CEO has public company as well as biopharma development and commercial experience • Robust IP portfolio, Platform validated through multiple Industry, government and university hospital partnerships • De - risked and cost - efficient business model structured to create significant value 4

Platform Validated by World Leading Partners RESEARCH CLINICAL TRIAL SITES 5

6 Management Team: Extensive Oncology and Drug Development Experience Veteran Operators with Public Company and IPO Experience • Drug delivery expertise Preclinical through Phase 3 • Public biotech company CEO experience • 25 years, multiple transactions • Titan Pharmaceutics, IPO Daniel Donovan CEO Rare Life Emer Leahy, Ph.D. CEO Psychogenics Mark A. Goldberg, MD Former President & COO of PAREXEL Lewis H. Bender CEO Intensity Lewis H. Bender, MIT ChE, MS, MA, MBA Founder, CEO John Wesolowski, MBA, CPA Chief Financial Officer, Principal Accounting Officer and Controller Brian Schwartz, MD Clinical Development CEO, CTO, VP, BD & Manufacturing CEO Manufacturing James M. Ahlers Executive Vice President - Corporate Finance CFO BOARD OF DIRECTORS KEY MANAGEMENT Ian Walters Medical Advisor Steve Innaimo Project Management Rebecca Drain, Doranne Frano Regulatory & Quality Rita Cooney PH.D. Analytical Chemistry Karen Du Clinical Operations Joseph Bernadino, George Klein Manufacturing
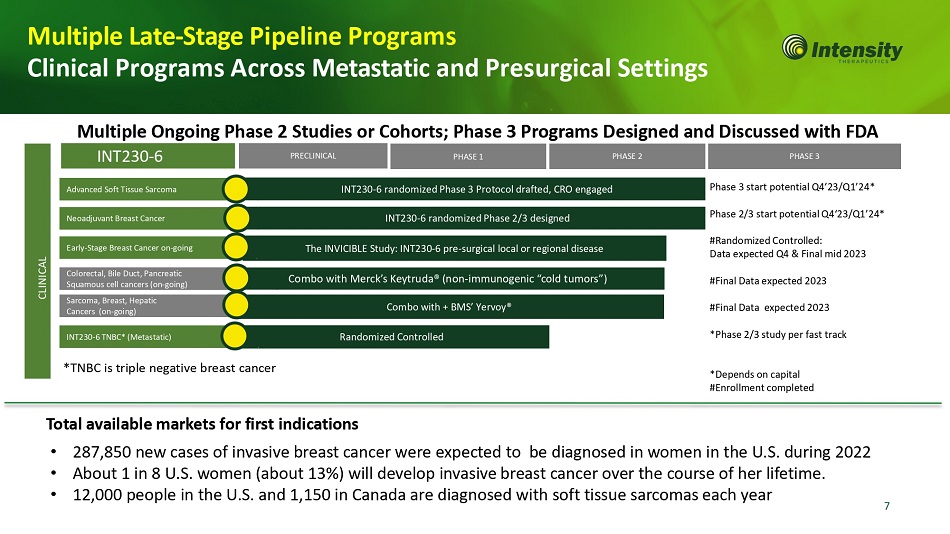
Advanced Soft Tissue Sarcoma INT230 - 6 randomized Phase 3 Protocol drafted, CRO engaged PHASE 3 PHASE 2 PHASE 1 PRECLINICAL INT230 - 6 Colorectal, Bile Duct, Pancreatic Squamous cell cancers (on - going) Sarcoma, Breast, Hepatic Cancers (on - going) Combo with + BMS’ Yervoy® Combo with Merck’s Keytruda® (non - immunogenic “cold tumors”) Multiple Late - Stage Pipeline Programs Clinical Programs Across Metastatic and Presurgical Settings Multiple Ongoing Phase 2 Studies or Cohorts; Phase 3 Programs Designed and Discussed with FDA The INVICIBLE Study: INT230 - 6 pre - surgical local or regional disease Early - Stage Breast Cancer on - going CLINICAL Phase 3 start potential Q4’23/Q1’24* Phase 2/3 start potential Q4‘23/Q1’24* #Randomized Controlled: Data expected Q4 & Final mid 2023 #Final Data expected 2023 #Final Data expected 2023 *Phase 2/3 study per fast track *Depends on capital #Enrollment completed *TNBC is triple negative breast cancer Randomized Controlled INT230 - 6 TNBC* (Metastatic) Neoadjuvant Breast Cancer INT230 - 6 randomized Phase 2/3 designed Total available markets for first indications • 287,850 new cases of invasive breast cancer were expected to be diagnosed in women in the U.S. during 2022 • About 1 in 8 U.S. women (about 13%) will develop invasive breast cancer over the course of her lifetime. • 12,000 people in the U.S. and 1,150 in Canada are diagnosed with soft tissue sarcomas each year 7

• Phase 3 programs - important market opportunities: Metastatic sarcoma : • 157,000 patients in US; • 12,000 new cases per year (6,000 deaths); (US) • Estimated annual revenue per patient based on phase 2 use Presurgical Breast cancer : First accelerated approval endpoints, then full approval • INT230 - 6 with Standard of Care (SOC) chemotherapy: 30,000 patients US • w/out chemotherapy: 60,000 Large tumor cases; (US) INT230 - 6 vs. no treatment (current SOC) 8 First Two Clinical Market Opportunities
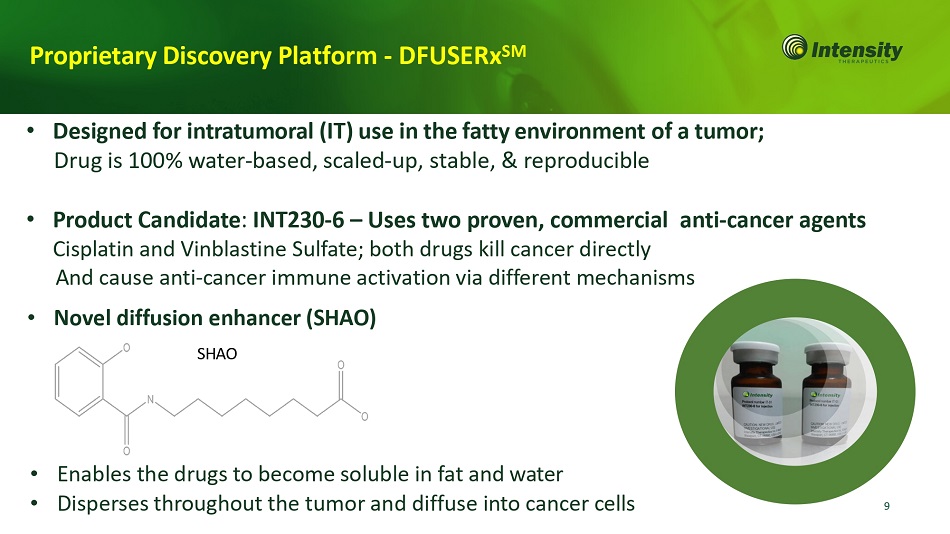
9 Proprietary Discovery Platform - DFUSERx SM • Designed for intratumoral (IT) use in the fatty environment of a tumor; Drug is 100% water - based, scaled - up, stable, & reproducible • Product Candidate : INT230 - 6 – Uses two proven, commercial anti - cancer agents Cisplatin and Vinblastine Sulfate; both drugs kill cancer directly And cause anti - cancer immune activation via different mechanisms • Novel diffusion enhancer (SHAO) SHAO • Enables the drugs to become soluble in fat and water • Disperses throughout the tumor and diffuse into cancer cells
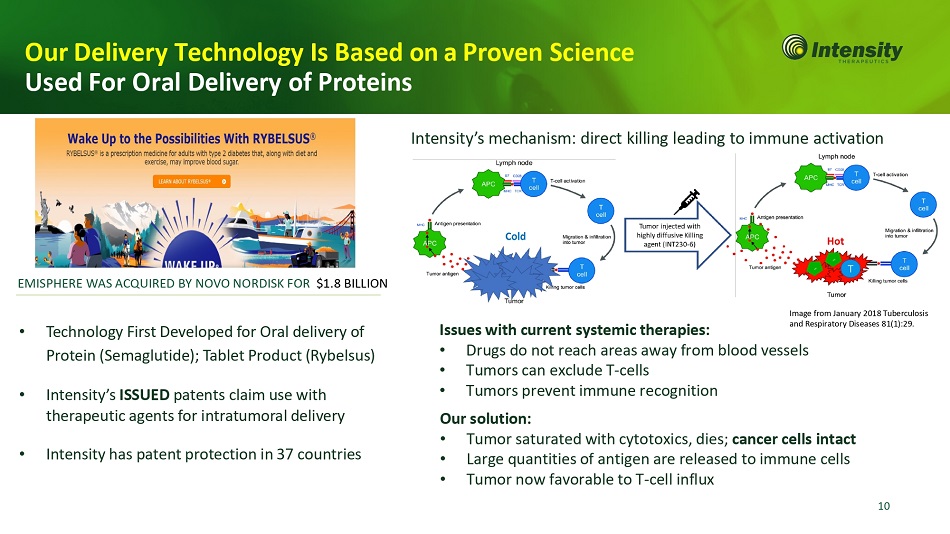
10 Our Delivery Technology Is Based on a Proven Science Used For Oral Delivery of Proteins • Technology First Developed for Oral delivery of Protein (Semaglutide); Tablet Product (Rybelsus) • Intensity’s ISSUED patents claim use with therapeutic agents for intratumoral delivery • Intensity has patent protection in 37 countries EMISPHERE WAS ACQUIRED BY NOVO NORDISK FOR $1.8 BILLION Issues with current systemic therapies: • Drugs do not reach areas away from blood vessels • Tumors can exclude T - cells • Tumors prevent immune recognition Our solution: • Tumor saturated with cytotoxics, dies; cancer cells intact • Large quantities of antigen are released to immune cells • Tumor now favorable to T - cell influx Image from January 2018 Tuberculosis and Respiratory Diseases 81(1):29. Intensity’s mechanism: direct killing leading to immune activation
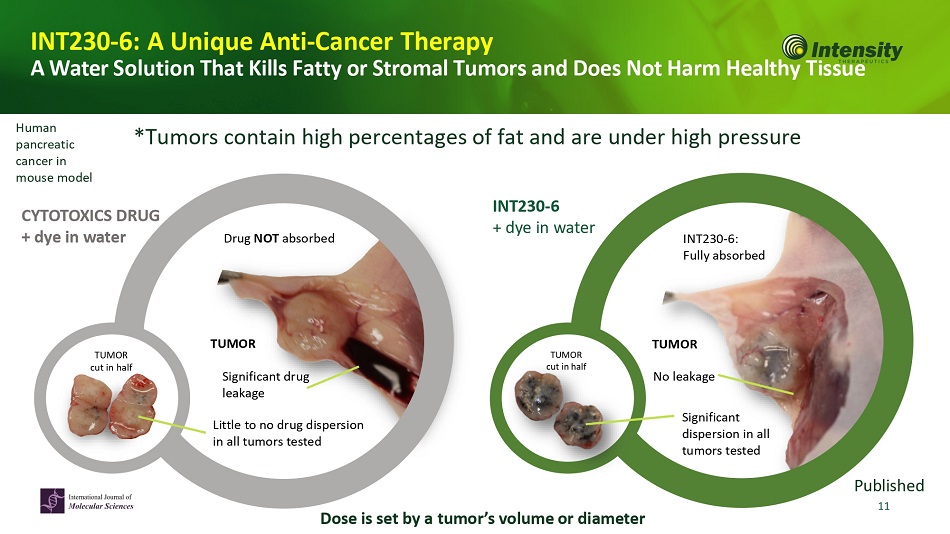
INT230 - 6: A Unique Anti - Cancer Therapy A Water Solution That Kills Fatty or Stromal Tumors and Does Not Harm Healthy Tissue *Tumors contain high percentages of fat and are under high pressure CYTOTOXICS DRUG + dye in water Little to no drug dispersion in all tumors tested TUMOR cut in half Significant drug leakage Drug NOT absorbed Human pancreatic cancer in mouse model TUMOR cut in half Significant dispersion in all tumors tested No leakage INT230 - 6: Fully absorbed INT230 - 6 + dye in water Dose is set by a tumor’s volume or diameter TUMOR TUMOR Published 11
12 Patients Enrolled: 91 – Complete INT230 - 6 R andomized to either no treatment or saline injection • Site: Ottawa Hospital • Investigator: Dr. Angel Arnaout • Objectives : Cause sufficient tumor necrosis prior to surgery to activate the immune system and determine INT230 - 6 safety presurgically • Final Goal: Reduce the risk of disease recurrence Our clinical results have been selected for Spotlight Oral Podium Presentation at: Design: Randomized, Placebo Controlled Phase 2 Window Trial In Presurgical Breast Cancer (BC): The INVINCIBLE Study The San Antonio Breast Cancer Society (SABCS) annual meeting December 2022:
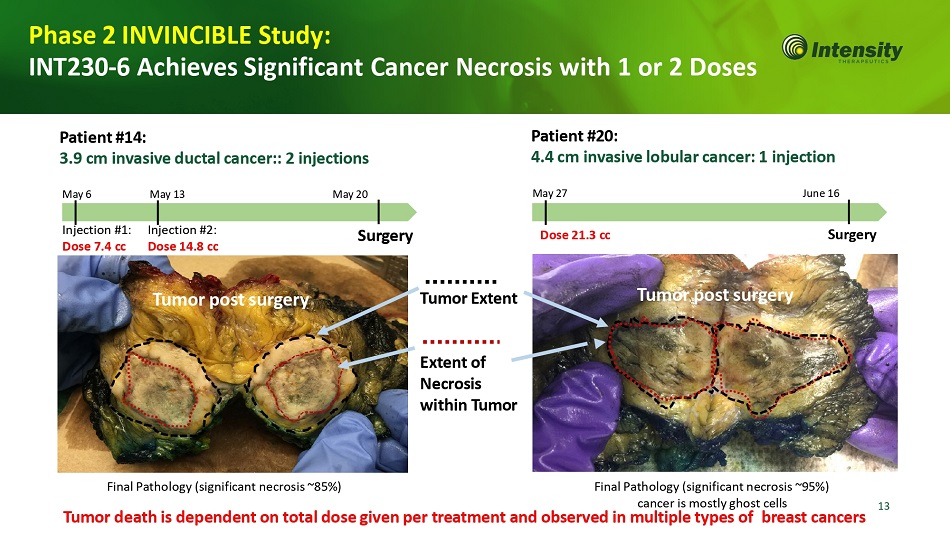
13 Tumor Extent Extent of Necrosis within Tumor Phase 2 INVINCIBLE Study: INT230 - 6 Achieves Significant Cancer Necrosis with 1 or 2 Doses Patient #14: 3.9 cm invasive ductal cancer:: 2 injections May 6 May 13 May 20 Final Pathology (significant necrosis ~85%) Final Pathology (significant necrosis ~95%) cancer is mostly ghost cells Tumor death is dependent on total dose given per treatment and observed in multiple types of breast cancers Injection #1: Dose 7.4 cc Injection #2: Dose 14.8 cc Surgery Patient #20: 4.4 cm invasive lobular cancer: 1 injection May 27 June 16 Dose 21.3 cc Surgery Tumor post surgery Tumor post surgery
INT230 - 6 had Favorable Safety in the Presurgical BC Setting • No surgery was delayed or cancelled • No surgical procedure was altered • No cosmetic differences noted • Mean wait time to surgery: 24 days (range 14 - 34 days) – normal timeframe • 89% of adverse events were grade 1; all resolved within 7 days • Patient interest in the drug and acceptability was high; accrual was rapid Pre vs. Post treatment (part1) • In tumor: increase in abundance of CD4+, CD8+, naïve T, B and NK T cells • In tumor microenvironment: increase in CD8 T, CD4 T, naïve and B cells • Over 200 immune cell genes activated 14
Study: Necrosis Efficacy and Phase 2/3 Study Design 15 Major pathological response (MPR) defined as < 10% residual cancer remaining in tumor • MPR was 6% overall in study with 14.3% in tumors >2.9 cm compared to control (0%) p=0.042 Pathological complete response (pCR) defined as 100% elimination of viable cancer (tumor + nodes) pCR was 9.5% in subjects with tumors >2.9 cm in diameter Design of Phase 3 Program in the larger T2, T3, T4 sized tumors INT230 - 6 + Standard of care (SOC is chemo/pembro) in TNBC and/or HER2+ vs. SOC • Accelerated approval using Pathological Complete Response (pCR); • Data 4 months post enrollment • Full approval showing event free survival (EFS); • Data 3 years post enrollment
IT - 01 Phase 1 / 2 Study in Metastatic Disease – Enrollment Complete ENROLLED: 110 16 Patients whose disease had progress after treatment with all approved therapies for their cancer, over 25 types of solid tumor types: Database now locked INT230 - 6 alone (64 patients) With Keytruda (30 patients) (includes 2 who finished monotherapy) With Yervoy (18 patients) • Injections up to 6 in a session into lung, liver, peritoneum, pancreas, breast, limbs, lymph, skin, muscles • Dosed started with 5 mL once per month. Current dose 175 mL every two weeks. Intensity’s results have been selected for Discussant Oral Podium Presentations at: ASCO (2) SITC • The Annual American Society of Clinical Oncology: • The Annual Society for the Immunotherapy of Cancer: • The Annual Connective Tissue Society (sarcoma): CTOS (2) Attacking the Tumors – Sparing the Patient
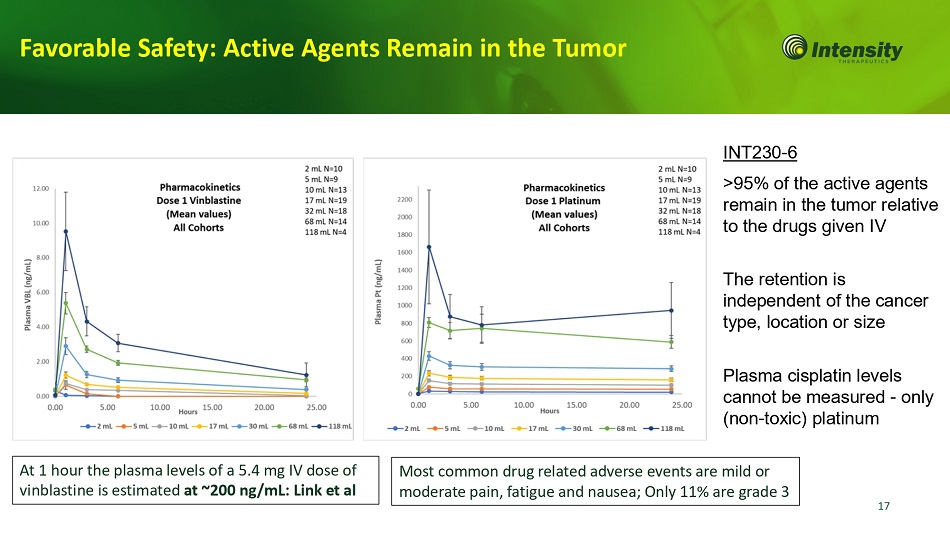
Favorable Safety: Active Agents Remain in the Tumor INT230 - 6 >95% of the active agents remain in the tumor relative to the drugs given IV The retention is independent of the cancer type, location or size Plasma cisplatin levels cannot be measured - only (non - toxic) platinum At 1 hour the plasma levels of a 5.4 mg IV dose of vinblastine is estimated at ~200 ng/mL: Link et al moderate pain, fatigue and nausea; Only 11% are grade 3 17 Most common drug related adverse events are mild or
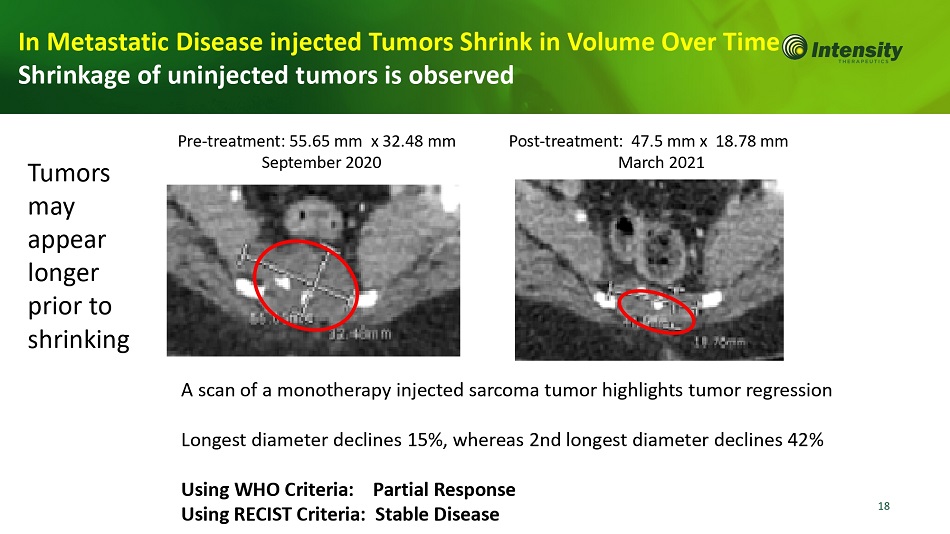
18 In Metastatic Disease injected Tumors Shrink in Volume Over Ti Shrinkage of uninjected tumors is observed A scan of a monotherapy injected sarcoma tumor highlights tumor regression Longest diameter declines 15%, whereas 2nd longest diameter declines 42% Using WHO Criteria: Partial Response Using RECIST Criteria: Stable Disease Pre - treatment: 55.65 mm x 32.48 mm September 2020 Post - treatment: 47.5 mm x 18.78 mm March 2021 Tumors may appear longer prior to shrinking
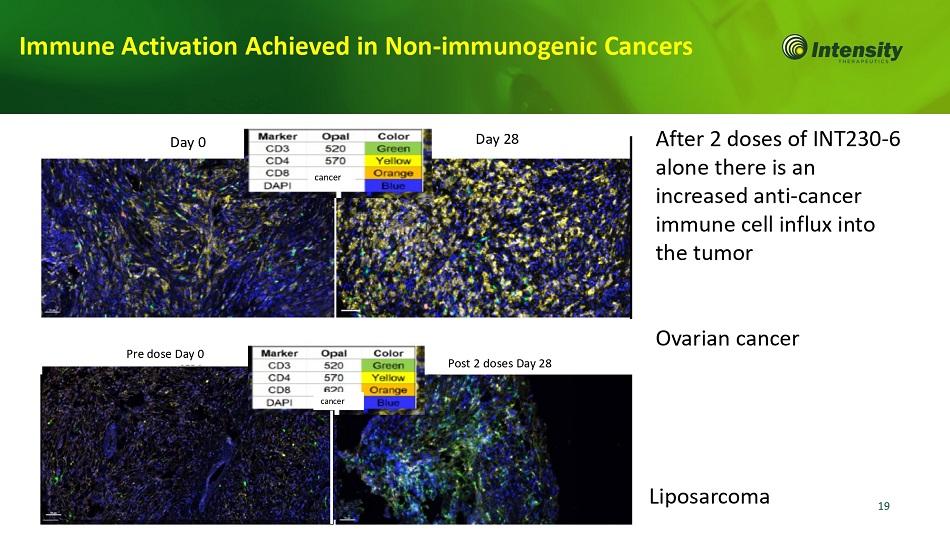
19 Post 2 doses Day 28 Pre dose Day 0 Liposarcoma cancer Immune Activation Achieved in Non - immunogenic Cancers After 2 doses of INT230 - 6 alone there is an increased anti - cancer immune cell influx into the tumor Ovarian cancer Day 0 Day 28 cancer
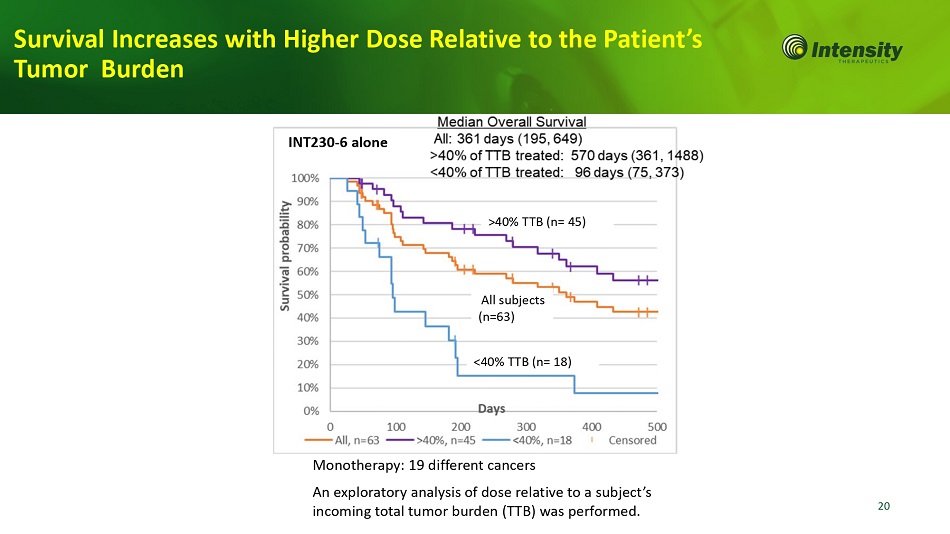
20 All subjects (n=63) >40% TTB (n= 45) <40% TTB (n= 18) INT230 - 6 alone Monotherapy: 19 different cancers An exploratory analysis of dose relative to a subject’s incoming total tumor burden (TTB) was performed. Survival Increases with Higher Dose Relative to the Patient’s Tumor Burden
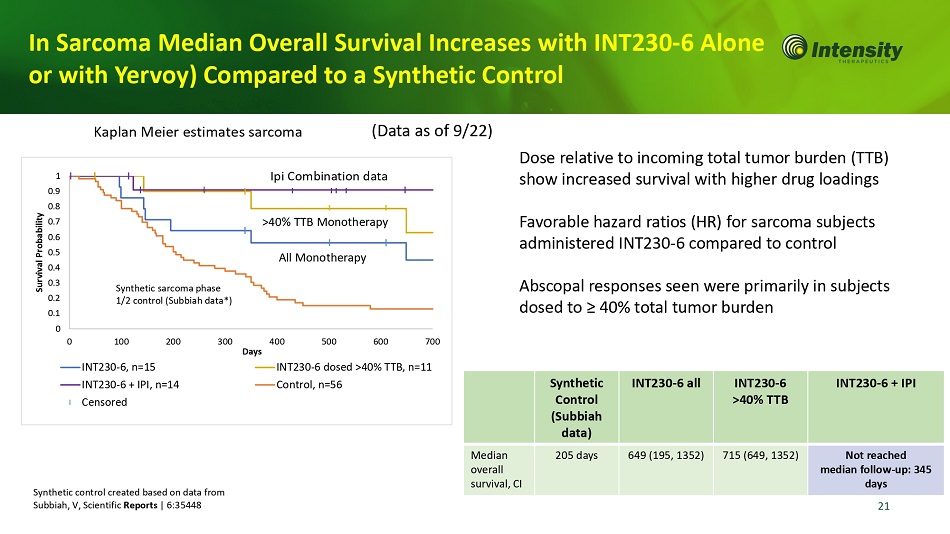
21 1 0.9 0.8 0.7 0.6 0.5 0.4 Survival Probability 0.3 Synthetic sarcoma phase 0.2 1/2 control (Subbiah data*) 0.1 0 0 100 200 300 400 500 600 700 Days INT230 - 6, n=15 INT230 - 6 dosed >40% TTB, n=11 INT230 - 6 + IPI, n=14 Control, n=56 Censored Kaplan Meier estimates sarcoma Ipi Combination data INT230 - 6 + IPI INT230 - 6 >40% TTB INT230 - 6 all Synthetic Control (Subbiah data) Not reached median follow - up: 345 days 715 (649, 1352) 649 (195, 1352) 205 days Median overall survival, CI Dose relative to incoming total tumor burden (TTB) show increased survival with higher drug loadings Favorable hazard ratios (HR) for sarcoma subjects administered INT230 - 6 compared to control Abscopal responses seen were primarily in subjects dosed to ≥ 40% total tumor burden In Sarcoma Median Overall Survival Increases with INT230 - 6 Alon or with Yervoy) Compared to a Synthetic Control Synthetic control created based on data from Subbiah, V, Scientific Reports | 6:35448 >40% TTB Monotherapy All Monotherapy (Data as of 9/22)
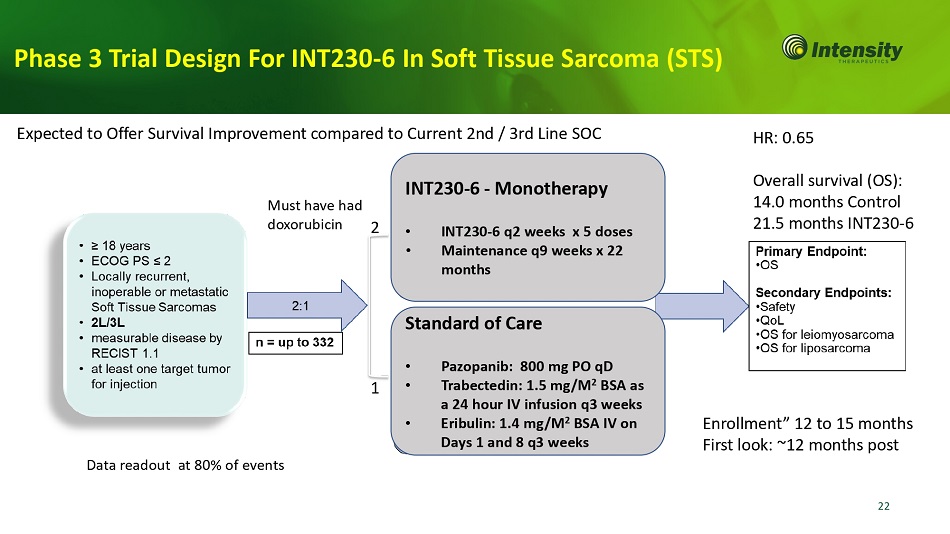
Must have had doxorubicin HR: 0.65 Overall survival (OS): 14.0 months Control 21.5 months INT230 - 6 Data readout at 80% of events Phase 3 Trial Design For INT230 - 6 In Soft Tissue Sarcoma (STS) INT230 - 6 - Monotherapy • INT230 - 6 q2 weeks x 5 doses • Maintenance q9 weeks x 22 months Standard of Care 22 • Pazopanib: 800 mg PO qD • Trabectedin: 1.5 mg/M 2 BSA as a 24 hour IV infusion q3 weeks • Eribulin: 1.4 mg/M 2 BSA IV on Days 1 and 8 q3 weeks 2 1 Enrollment” 12 to 15 months First look: ~12 months post Expected to Offer Survival Improvement compared to Current 2nd / 3rd Line SOC
• INT230 - 6 represents a new treatment approach to solid tumors (immunological cell killing) both in the metastatic and presurgical (neoadjuvant) settings • Strong interest from: academic hospitals, major clinical oncology societies, big pharma and government • INT230 - 6 has: • induced significant necrosis in large tumors following a single dose • Immune activation observed of non - immunogenic cancer types • Shown favorable safety and promising increased survival efficacy 23 Conclusions
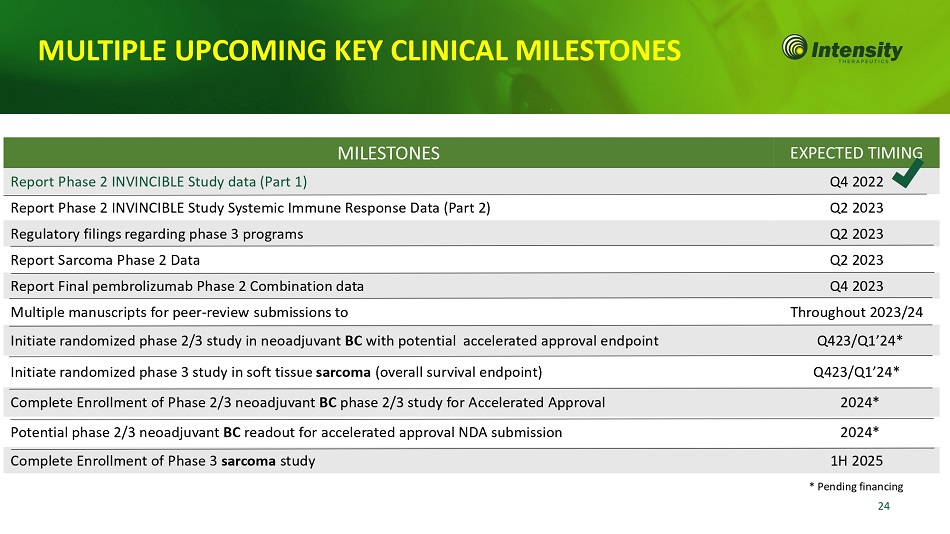
MULTIPLE UPCOMING KEY CLINICAL MILESTONES MILESTONES EXPECTED TIMING Report Phase 2 INVINCIBLE Study data (Part 1) Q4 2022 Report Phase 2 INVINCIBLE Study Systemic Immune Response Data (Part 2) Q2 2023 Regulatory filings regarding phase 3 programs Q2 2023 Report Sarcoma Phase 2 Data Q2 2023 Report Final pembrolizumab Phase 2 Combination data Q4 2023 Multiple manuscripts for peer - review submissions to Throughout 2023/24 Initiate randomized phase 2/3 study in neoadjuvant BC with potential accelerated approval endpoint Q423/Q1’24* Initiate randomized phase 3 study in soft tissue sarcoma (overall survival endpoint) Q423/Q1’24* Complete Enrollment of Phase 2/3 neoadjuvant BC phase 2/3 study for Accelerated Approval 2024* Potential phase 2/3 neoadjuvant BC readout for accelerated approval NDA submission 2024* Complete Enrollment of Phase 3 sarcoma study 1H 2025 * Pending financing 24
Investment Highlights • Novel Approach to Immuno - Oncology with First - in - Class Compound that causes cancer cell death leading to an immune response for indications with high unmet medical need • Multiple Late - Stage Pipeline Programs in the Clinic across metastatic and presurgical settings with multiple near - term inflexion points • Experienced Leadership Team from Emisphere, Roche and Bristol Myers; CEO has public company as well as biopharma development and commercial experience • Robust IP portfolio, Platform validated through multiple Industry, government and university hospital partnerships • De - risked and cost - efficient business model structured to create significant value 25

INTENSITY THERAPEUTICS 26 A NEW WEAPON IN THE WAR ON CANCER Contact Investor Relations Contact : Rx Communications Group Michael Miller (917) - 633 - 6086 mmiller@rxir.com Thank you!

Intensity Therapeutics A New Weapon In The War On Cancer Appendix slides 27
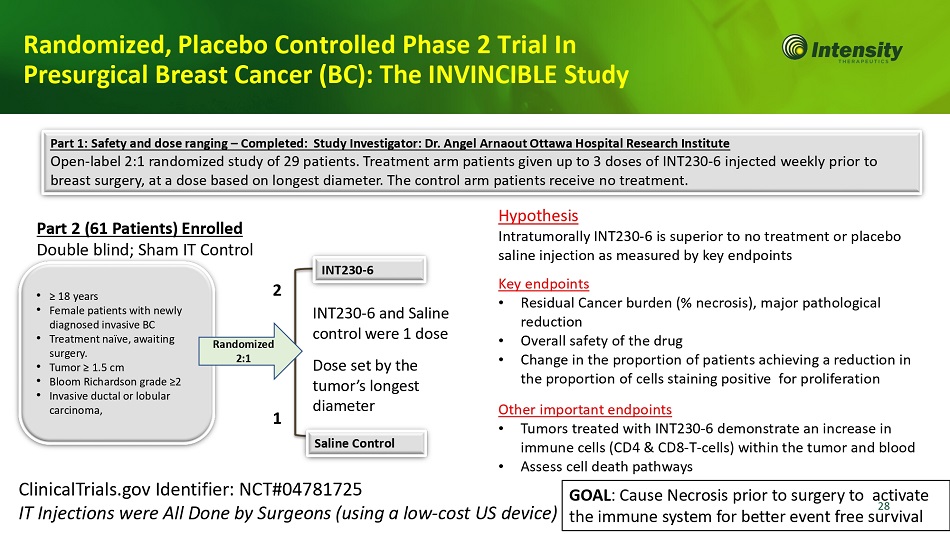
28 • ≥ 18 years • Female patients with newly diagnosed invasive BC • Treatment naïve, awaiting surgery. • Tumor ≥ 1.5 cm • Bloom Richardson grade ≥2 • Invasive ductal or lobular carcinoma, Randomized 2:1 INT230 - 6 Saline Control Part 1: Safety and dose ranging – Completed: Study Investigator: Dr. Angel Arnaout Ottawa Hospital Research Institute Open - label 2:1 randomized study of 29 patients. Treatment arm patients given up to 3 doses of INT230 - 6 injected weekly prior to breast surgery, at a dose based on longest diameter. The control arm patients receive no treatment. ClinicalTrials.gov Identifier: NCT#04781725 IT Injections were All Done by Surgeons (using a low - cost US device) INT230 - 6 and Saline control were 1 dose Dose set by the tumor’s longest diameter • Residual Cancer burden (% necrosis), major pathological reduction • Overall safety of the drug • Change in the proportion of patients achieving a reduction in the proportion of cells staining positive for proliferation Hypothesis Intratumorally INT230 - 6 is superior to no treatment or placebo saline injection as measured by key endpoints Key endpoints Other important endpoints • Tumors treated with INT230 - 6 demonstrate an increase in immune cells (CD4 & CD8 - T - cells) within the tumor and blood • Assess cell death pathways Randomized, Placebo Controlled Phase 2 Trial In Presurgical Breast Cancer (BC): The INVINCIBLE Study Part 2 (61 Patients) Enrolled Double blind; Sham IT Control 2 1 GOAL : Cause Necrosis prior to surgery to activate the immune system for better event free survival
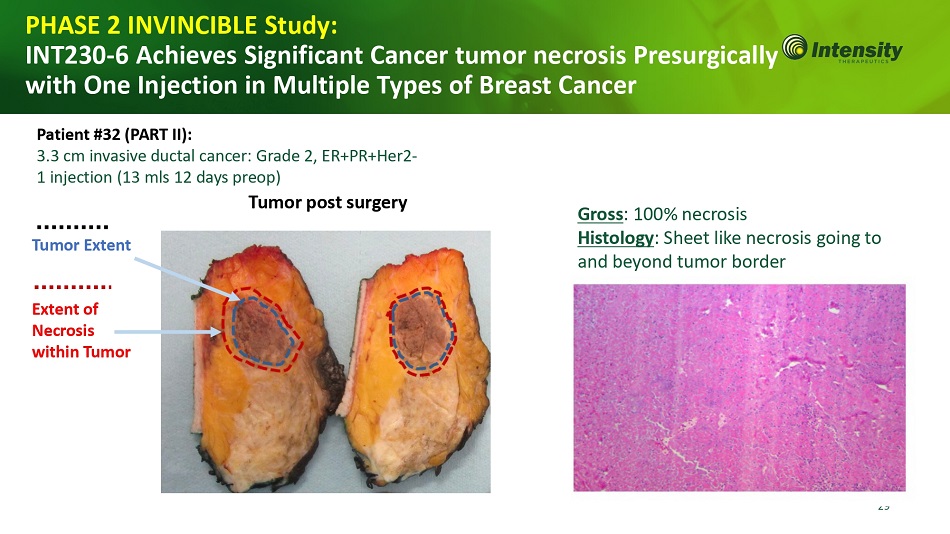
PHASE 2 INVINCIBLE Study: INT230 - 6 Achieves Significant Cancer tumor necrosis Presurgically with One Injection in Multiple Types of Breast Cancer Patient #32 (PART II): 3.3 cm invasive ductal cancer: Grade 2, ER+PR+Her2 - 1 injection (13 mls 12 days preop) Gross : 100% necrosis Histology : Sheet like necrosis going to and beyond tumor border Tumor Extent Extent of Necrosis within Tumor Tumor post surgery 29
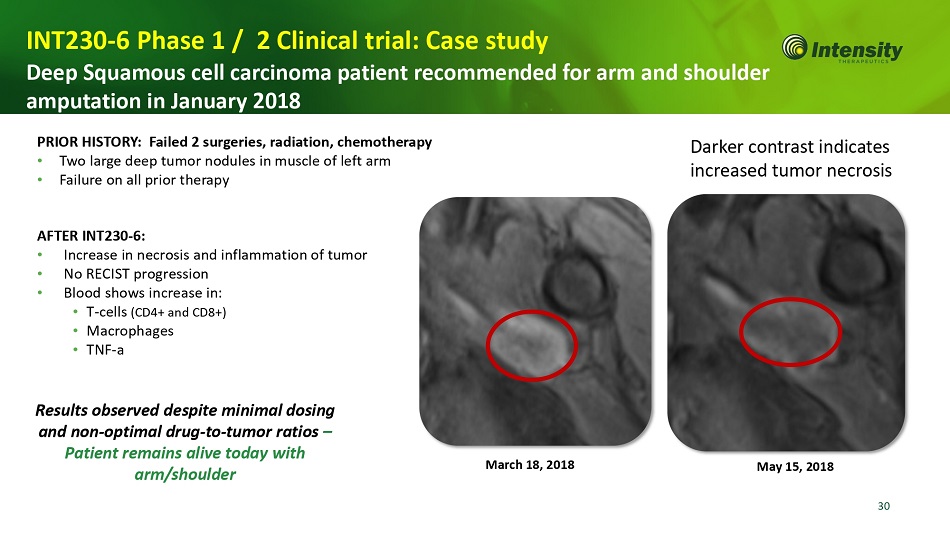
INT230 - 6 Phase 1 / 2 Clinical trial: Case study PRIOR HISTORY: Failed 2 surgeries, radiation, chemotherapy • Two large deep tumor nodules in muscle of left arm • Failure on all prior therapy AFTER INT230 - 6: • Increase in necrosis and inflammation of tumor • No RECIST progression • Blood shows increase in: • T - cells (CD4+ and CD8+) • Macrophages • TNF - a Results observed despite minimal dosing and non - optimal drug - to - tumor ratios – March 18, 2018 May 15, 2018 Darker contrast indicates increased tumor necrosis 30 Patient remains alive today with arm/shoulder Deep Squamous cell carcinoma patient recommended for arm and shoulder amputation in January 2018
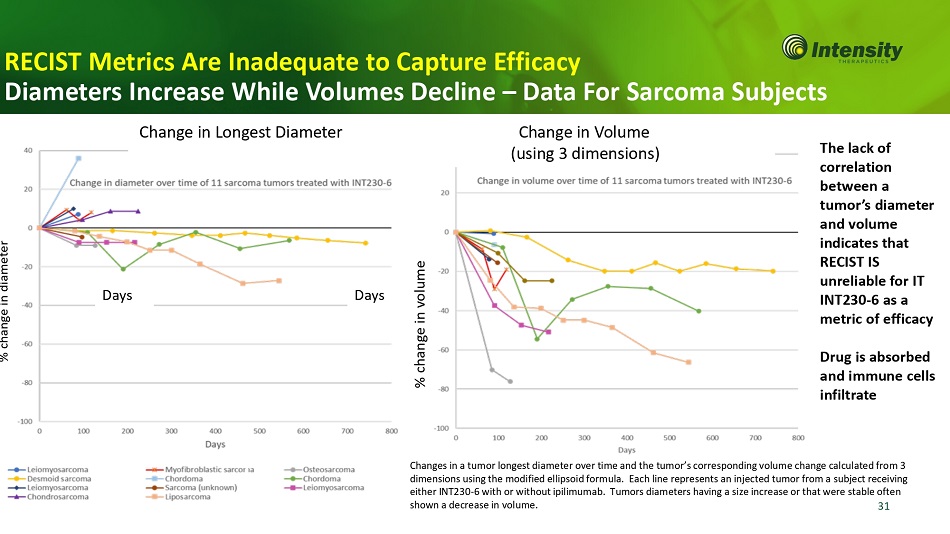
31 Change in Longest Diameter Change in Volume (using 3 dimensions) The lack of correlation between a tumor’s diameter and volume indicates that RECIST IS unreliable for IT INT230 - 6 as a metric of efficacy Drug is absorbed and immune cells infiltrate Days % change in diameter % change in volume Days Changes in a tumor longest diameter over time and the tumor’s corresponding volume change calculated from 3 dimensions using the modified ellipsoid formula . Each line represents an injected tumor from a subject receiving either INT 230 - 6 with or without ipilimumab . Tumors diameters having a size increase or that were stable often shown a decrease in volume. RECIST Metrics Are Inadequate to Capture Efficacy Diameters Increase While Volumes Decline – Data For Sarcoma Subjects
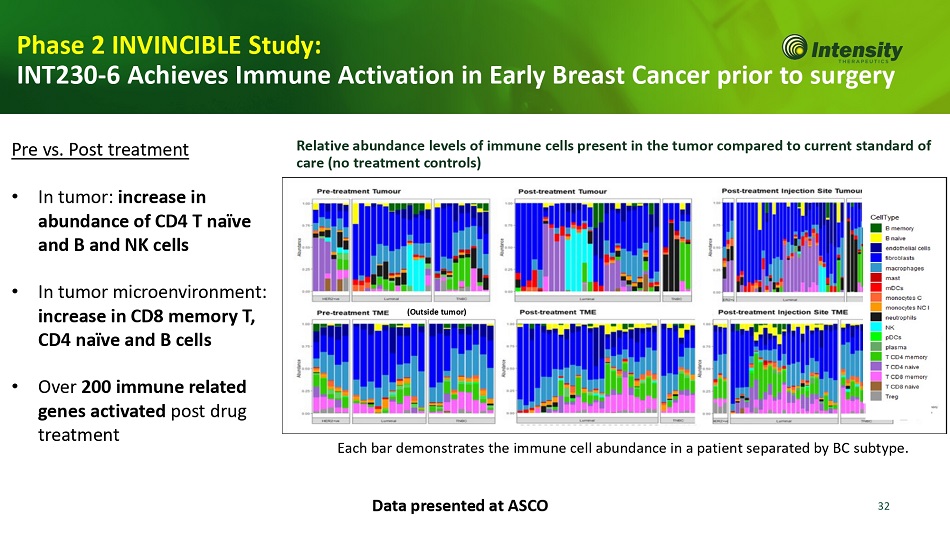
32 Phase 2 INVINCIBLE Study: INT230 - 6 Achieves Immune Activation in Early Breast Cancer prior to surgery Relative abundance levels of immune cells present in the tumor compared to current standard of care (no treatment controls) Each bar demonstrates the immune cell abundance in a patient separated by BC subtype. Data presented at ASCO (Outside tumor) Pre vs. Post treatment • In tumor: increase in abundance of CD4 T naïve and B and NK cells • In tumor microenvironment: increase in CD8 memory T, CD4 naïve and B cells • Over 200 immune related genes activated post drug treatment
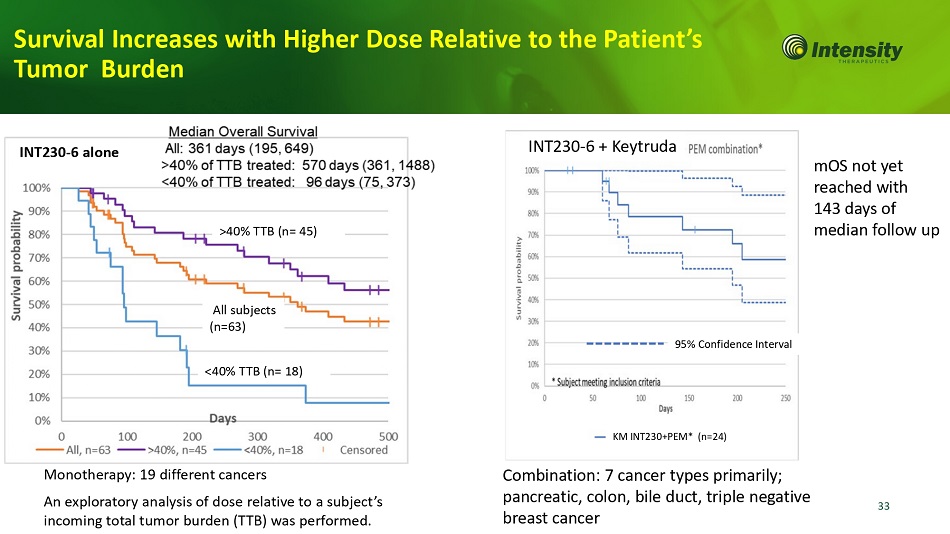
33 All subjects (n=63) >40% TTB (n= 45) <40% TTB (n= 18) KM INT230+PEM* (n=24) INT230 - 6 alone mOS not yet reached with 143 days of median follow up Monotherapy: 19 different cancers An exploratory analysis of dose relative to a subject’s incoming total tumor burden (TTB) was performed. INT230 - 6 + Keytruda Combination: 7 cancer types primarily; pancreatic, colon, bile duct, triple negative breast cancer 95% Confidence Interval Survival Increases with Higher Dose Relative to the Patient’s Tumor Burden